"Basic
Therapy" - The Complex Development of the Nervous system -
In.: Developmental Pedagogy (Fejlesztő Pedagógia), Budapest, 1994/4-5.
Translated by Gabor Toth (2000)
Abstract
The
"Basic Therapy" Foundation’s method is the complex development of the
nervous system, guided by motion patterns in succession of movement models. By
using this form of therapy, minimal brain injury, attention deficit and
hyperactivity disorder (ADHD, HAHAS or POS), mental retardation and
developmental dyslexia can be influenced and sometimes even totally corrected.
Our therapy is based on programs first developed by the neurologist Carl
Henry Delacato, the neurosurgeon Temple Fay, as well as the physical therapist
Glenn Doman. But even though these scientists have been at the origin of
the therapy, we have been completing and wholly transforming the program
into the "Basic Therapy", by using the basic studies and combining
them with the therapeutically results and findings of the last years. The
"Basic Therapy" supported by our foundation today is mainly influencing
the brain of the child in the area where the problem has been located previously.
We therefore based our method on the fact that every child is born with
approx. 12 thousand million brain cells and will use only 10 percent of
these during lifetime.
Thus, our aim is to activate the so-called "dormant" cells and to
lead them to take over the function of the damaged or immature cells. This
progression in taking over can be easily followed by the watch of the movement
development which continues until the pathway is fully matured, utilising all
levels of the brain. The result is that the child i.e. can read fluently, can
move as she/he can and well enough to take its place in society alongside with
other children who are fully accepted in the world as a "normal"
child or person. Due to the ever continuing gathering of results and the
comparison with other findings during the process of individual therapy, we are
constantly developing the forms and tools of "Basic Therapy".
Our foundation helps to organise the constant exchange between the children
under therapy and their parents on the one hand, as well as with the scientists
following the projects on the other hand. We therefore finance the consultancy
to parents as well as the education and training of scientists in the method
of "Basic Therapy". In the future, we intend to create a centre
of exchange and therapy in Budapest in order to popularise "Basic
Therapy" and to open it to those who did not know a solution to their
child’s problem until today.
In order to succeed in this matter, we would need financial and moral support.
The children and their parents would be most grateful if anyone could help. In
case of any question we would be very happy to provide you with further
information.
Address:
BASIC THERAPY Foundation
Budapest, Harrer P. u. 10.
Hungary-1033.
P.O. Box: Budapest, Pf.701.
1535-Hungary
Account Number:
BB 10104105-56095046-00000001
"Basic Therapy"
-Psychomotor Therapy based on sensorimotor development-
Translated by Gabor Toth, M.Ed.
(Translated and edited from: “Basic Therapy”,
Scientific Study, Basic Therapy Association, Budapest, 1999.)
Introduction part:
This paper was written as a Training Guide of postgraduate studies for special
teachers, psychologists, ST and PT (mainly connected to dyslalia, dysphasia,
dyslexia and LD). The aim of this paper is "how we can
use the scientific results of the neuro-psychology in the special
education". The "Basic Therapy" Foundation (Hungary)
is a group of different professionals (neurologist, psychiatrist,
ophthalmologist, psychologist, ST, PT, Pető-conductor, special school teacher
etc.) who want to make a complex developmental therapy, what's may effect the
nervous system by making new and stable synapses-net (pathway) across the
development of the movement co-ordination-system. This method is a Psychomotor
Therapy dominated by sensorimotor development, guided by motion
patterns in succession of the human movement models. By using this form of a
developmental therapy minimal brain injury (MBI), attention deficit and
hyperactivity disorder (ADHD), mental retardation (MR) and developmental
dyslexia/dysgraphia (DD) could be influenced and sometimes even totally
corrected.
Our therapy is based on a program what was first developed by a neurologist
C.H. Delacato, a neurosurgeonTemple Fay
and a physical therapist Glenn Doman at the Philadelphia Rehabilitation
Centre in the 60's. But even thought these scientists have been at the origin
of the therapy, our Foundation have been completing and wholly transforming the
program into the present Psychomotor Therapy, by using the basic studies and
combining them with the therapeutically results and findings of the last years.
We based our method on the fact that every child is born with approximately 12
thousand million brain cells and will use only 10% of these during lifetime.
Thus, our aim is to activate the so-called "dormant-cells" and to lead
them to take over the function of the damaged or immature cells. This
progression in taking over can be easily followed by the observation of the movement
development, which continues until the pathway is fully matured, utilising
all levels of the brain. The result is that the child i.e. can read fluently,
can move as s/he can and well enough to take its place in society alongside
with other children, which are fully accepted in the word as a
"normal" child. Due to the ever-continuing gathering of result and
the comparison with other findings during the process of individual therapy, we
are constantly developing the forms and tools of this method.
First part:
Disorders of language development, what will effect the learning ability?
The most frequent speech disorders are those that disturb the child's
acquisition or learning of language. While those concerned with modern
terminology are striving for an improved classification according to the
etiologic (causative) factors, it is still customary to classify these
disorders on the basis of the complaint: absence of speech, baby talk, poorly
intelligible articulation, lisping, etc. Recent studies of large numbers of
children with such developmental language disorders have shown that at least
two chief classes of these disorders may be distinguished:
1. General language disability from genetic factors with a familial (inherited)
pattern chiefly from the paternal side, and acquired language disorders due to
damage sustained before, during or shortly after birth (i.e. perinatally).
These latter perinatal damages encompass the gamut of toxic, infectious,
traumatic, nutritional, hormonal and other damages that may hurt the growing foetus
or young infant.
2. Hereditary factors also encompass a great variety of genetically
predetermined influences, including:
- familial tendency to exhibit slow language development, lesser endowment in
the brain area for language, inferior function in the highest brain areas of
auditory performance without organic damage to the ears, slow maturation of
motor function (including clumsiness and deviation from normal cerebral
dominance), and other signs of delayed cerebral growth. Additional
environmental causes include poor language patterns used by the family,
parental neglect, emotional maladjustment, general weakness from prolonged
disease, as well as various socio-economic, cultural and other psychological
influences.
While some otherwise perfectly normal children (particularly boys) may not
elect to begin talking until age three, making good progress in every respect
from then on. The absence of speech after age two may be caused by any of the
conditions mentioned thus far and would appear to merit prompt investigation.
If an organic cause can be detected, the symptomatic description of
delayed language development then yields to a specific etiologic (causal)
diagnosis. Although, it is best to describe the absence of speech in early
childhood as simply delayed language development. Some American investigators
tend to refer to this condition as congenital (present at birth) aphasia, a
term rejected by most European scholars who argue that there cannot be an
inborn or early acquired aphasia before a language has been learned (so called
dysphasia).
Many children encounter unusual difficulties in mastering the patterns of
articulation (what is one of the most difficult sensor-integration movement) of
their mother tongue and are said to manifest articulatory immaturity (infantile
dyslalia). If no organic cause can be found, the probable cause may
be delayed maturation of psychomotor skills. Marked delays of language
development are often followed by a period of inability to learn the rules of
grammar and syntax at the usual age (dysgrammatism and the cause usually LD).
Though this is often a sign of inherited language disability, it may reflect mental
retardation or other types of brain damage. Some children who have suffered
such laboured language development may then go through a period of retarded
reading and writing disability, a condition often defined as dyslexia.
We would like to emphasize, that there are two chief varieties of it:
1. The primary or developmental reading and writing disability due to
constitutional (organic) and hereditary factors.
2. And a large secondary group of symptomatic reading disorders acquired
through any of the influences that retard language development in general,
including troubles with vision (that's why our team is working together with ophthalmologist
and we consult in every case).
Practically all investigators agree that primary or developmental dyslexia
shows a marked hereditary tendency (is familial) and is typically associated
with other disorders of psychomotor development, deviation from
the prevalent right handedness and poor function in the auditory area in the
brain, often associated with lack of musical talent. Primary dyslexia is
significantly associated with other developmental speech disorders.
Language and dyslexia
The language area of the brain surrounds the Sylvian fissure (see figure 1.) in
the dominant hemisphere.
Figure 1.
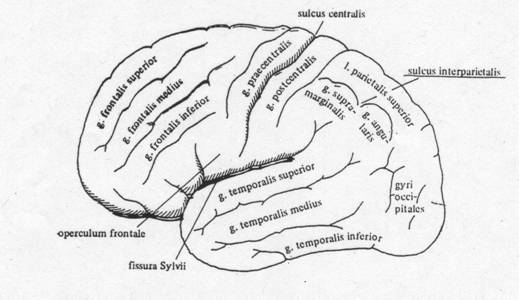
This area is divided
into two major components named after the pioneers Paul Broca and
Carl Wernicke. Broca's area lies in the third frontal
convolution, just anterior to the face area of the motor cortex and just
above the Sylvian fissure. This is often described as the motor, or
expressive, speech area; damage to it results in Broca's aphasia what in
the case of children called dysphasia. A language disorder characterised by
deliberate, telegraphic speech with very simple grammatical structure though
the speaker may be quite clear as to what he wishes to say and may communicate
successfully. Wernicke's area is in the superior part of the posterior temporal
lobe. It is close to the auditory cortex and is classically considered to be
the receptive language, or language comprehension, centre. A child who has maturity
problem or minimal brain damage in this area, or the patient with Wernicke's
aphasia has difficulty understanding language. His own speech is typically
fluent but is empty of content and characterised by circumlocutions, a high
incidence of vague words like "thing," and sometimes neologisms and
senseless "word salad." The entire posterior language area extends
into the parietal lobe and is connected to Broca's area by a fibre tract called
the arcuate fasciculus. Damage to this tract has been implicated in conduction
aphasia (or dysphasia), a disorder in which the patient can understand and
speak but has difficulty in repeating what is said to him. The suggestion is
that, in this condition, language can be comprehended by the posterior zone and
spoken by the anterior zone, but it can not be easily shuttled from one to the other.
It is important to note that dysphasia and aphasia is a disorder of language
and not of speech (although a dyspraxia/apraxia of speech, in which the programming
of motor speech output is affected, may accompany dysphasia/aphasia). The
writing and reading of dysphasic/aphasic child or adult patients, therefore,
usually commits the same type of error as their speech, while the reverse is
not the case. Isolated disorders of writing (dysgraphia) or more commonly,
reading (dyslexia) may occur as well, but these reflect a disruption of the
additional processing required for these activities over and above that
required for language.
One particular form of dyslexia deserves mention, as it is a clear example of a
disconnection syndrome a disorder resulting from the disconnection of two areas
(by the corpus callosum on Figure down) of the brain rather than from damage to
a "centre." This is dyslexia without dysgraphia, or letter-by-letter
reading, so called because it is not associated with writing disturbance and
because the patients tend to attempt to read by spelling words out loud letter
by letter. It usually results from a lesion in the posterior part of the left
hemisphere that disconnects the visual areas (on Figure 2.) of the brain from
the language areas. Also important the limbic system, what has important task
in balance and attention.
Figure 2.
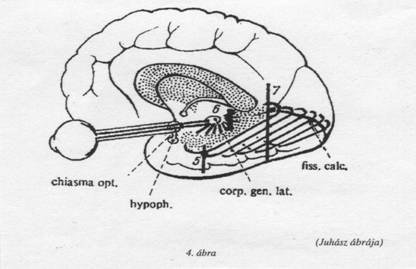
This renders the language areas effectively blind, so that they cannot be brought
to bear on visible language such as the written word. Writing is unaffected
because the right hand is still connected to the left hemisphere, and if
letters can be spoken out loud correctly (which is not always the case), the
child will be able to hear himself say them and reintegrate them into words.
Disconnection syndromes are an important concept in understanding behavioural
disorders (e.g. in the case of ADHD) associated with brain damage. The
possibility that deficits are caused by disconnection must always be borne in
mind.
Second part:
Why we use movement patterns to develop or re-develop the nervous system
The first answer in our life is the motor-answer; our first communication is
the motor-communication. It means that our movement developmental process is
the firs and fundamental communication with the close environment. Later all
other communication-forms are based on this. Piaget's theory said that the
first human measurable intelligence is the sensorimotor-intelligence and after
from this developing all the next level. Motor skills are
generally more easily remembered than are verbal skills. Researchers theorise
that this greater retention is due to the fact that motor skills are more
likely to be over-learned (repeated more often) than are verbal skills. The
factor that most influences motor ability is chronological age. Subjects
generally grow more proficient from the age of 4-5 until the end of 16-20's
(individually differences), when their abilities plateau for a few years and
then slowly decline. That is the reason why we usually start a therapy at age
of 4 or mostly 5 and the oldest child is around 16-17 years old.
The mechanisms of learning and remembering seem to depend on relatively
enduring changes in the nervous system. Apparently the effects of
learning are first retained in the brain by some reversible process, after
which a more permanent neural change takes place. Two types of neurological
processes have therefore been suggested. The short-term function of memory,
temporary and reversible may be achieved through a physiological mechanism
(e.g., synaptic electrical or chemical change) that keeps the memory
trace alive over a limited period of time. The ensuing, more permanent
(long-term) storage may depend on changes in the physical or chemical structure
of neurones; synaptic changes seem to be particularly important.
Human psychomotor skills are organised patterns of muscular activities
guided by changing signals from the environment. E.g. driving a car and
eye-hand co-ordination tasks such as drilling a tooth, throwing a ball, typing
or writing and playing a trombone are behavioural examples. Also called sensorimotor
and perceptual-motor skills, they are studied as special topics in the
experimental psychology of human learning and performance. In research
concerning psychomotor skills, particular attention is given to the learning
of co-coordinated activity of the arms, hands, fingers, and feet. (The
cerebral connections of the Human movement model and its Figure 3.)
Figure
3.
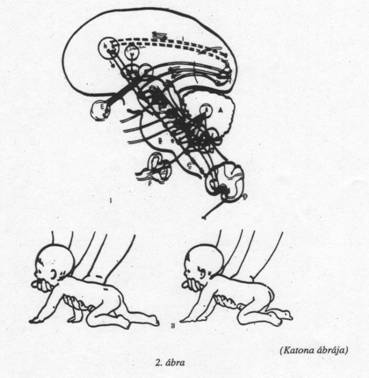
Psychomotor habits are mediated primarily by the sensory and motor
cortex of the brain and by the neural fibres (commissures) that connect the
two cerebral hemispheres. According to the majority of theoreticians, learning
proceeds as a mathematical function of the amount or duration of rewarded
(reinforced) practice. To acquire and perform such complex skills, a person
must closely monitor sensory stimulation. One may need to use visual
cues to judge the velocity and trajectory of an approaching object, or monitor
the pressure applied by one's own muscles. Hence, the term sensorimotor
skill reflects the idea that sensory and motor information must be
integrated to accomplish such acts. Motor acts occur automatically, such as
blinking the eyes or retracting a finger from a hot surface. Many human motor
skills, however, require practice. Such seemingly elementary skills as
walking, eating, and dressing must be mastered through practice by every child.
That is what we start from the beginning in our form of therapy, to build a
developmental line from the basic baby movement to a complex
motor-co-ordination movement.
Acquiring a motor skill is thought to involve three distinct stages. In the
first, called the cognitive stage, the person must comprehend the task
requirements. Studies demonstrate that those individuals who were pre-trained
with a verbal or illustrative description of the task were more likely to
master the skill. During the second or intermediate stage, the individual must
apply already acquired motor skills to the new task, master the motor skills
unique to that task, and integrate the two to avoid inappropriate and
unnecessary movements. In the final stage the skill becomes automat zed,
freeing the performer from thinking about each step of the process and
minimising dependence on external cues. Fluid execution of motor skills on the
part of accomplished performers has led researchers to think that sensorimotor
skills are enacted via a motor program, a blueprint for the entire
motor act, not just the sequencing of elements. This is well illustrated by the
phenomenon of co-articulation. Speech production of the letter "b" in
bat is different from the production of the "b" in beat. For such a
distinction to occur, the brain must be aware that one "b" is
followed by an "a" and that the other is followed by an
"ea", suggesting a preconceived plan for the whole utterance.
As motor skills are attained, changes in attention to sensory cues and
changes in reliance on feedback take place. While beginners rely mostly on
external cues, someone who has mastered a skill will rely more on internal
sources of feedback, such as those provided by muscles.
The kind of formal instruction that aids most in perfecting motor skills varies
for the early and later stages of acquisition. During the initial
stages, the most essential factors for learning are perceptual awareness, an
understanding of spatial relations and comprehension of mechanical principles.
Later, motor abilities such as speed of reaction, speed of movement and
co-ordination become critical. Retention of motor skills appears to be
most dependent upon the degree to which the skill was perfected, rather than
upon other variables such as the conditions under which it was learned. If a
skill has been over learned, exceeding a particular criterion,
retention will be better than if such levels had not been reached initially.
Third part
The process of the examination:
* neurological examination (by a neurologist)
* ophthalmologic examination (by an ophthalmologist)
* hearing examination (by an audiologist or ST)
* Gestalt examination
* examination of memory (visual, hearing, tactile, movement)
*movement examination, includes fine-motorium,
eye/hand-co-ordination(visual-motor-co-ordination), movement-reproduction etc
* reading and writing ability examination (only for school age children)
* pre-school examination (for 4-5 years old children)
* body scheme (left-right, examination of finger-praxis)
* constructive-praxis
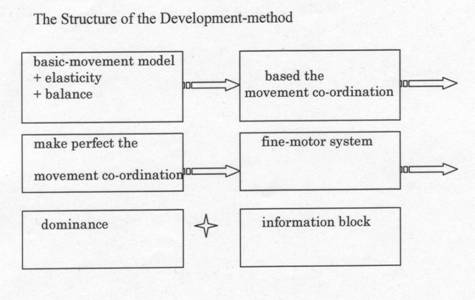
The Structure of the Development-method (Figure 4.)
Figure 4.
Last part
The groups of exercises:
1. "big" movements
2. elasticity (jumping, bounding)
3. balance
4. accustoming movements
5. cross patterns
6. fine-motor exercises
7. development of dominant hand
8. development of dominant leg
9. eye-exercises, development of eye-dominance, eye-hand co-ordination
10. position changing in space, movement-reproduction, space-orientation (3D)
11. body-scheme, finger-recognition, left-right/up-down orientation (2D)
12. constructive-praxis
13. hearing-exercises
14. kinaesthesia and sensor-turn over exercises (e.g. tactile »» visual)
15. memory exercises
16. Gestalt
17. warming up exercise
18. exercise of respiration
19. self-control exercises
20. rhythm exercise
21. speech-rhythm
22. neuro-habilitation exercises made by Lurija
23. time orientation
24. comprehension of context
25. sport exercise
26. movement seriality (sequence) exercise
27. ball-therapy
28. cross patterns for body-axis
29. open
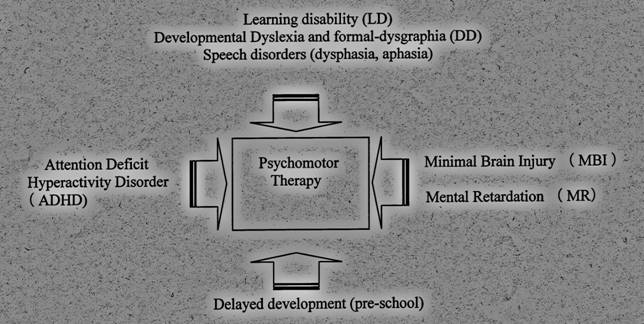
We use this form of Psychomotor Therapy in different cases what are connected
to the problem of the nervous system. We have different groups and every
different group has their own therapist whom educated and well experienced.
Our groups are:
* Learning disability (LD)
* ADHD
* Mental retardation
* Developmental dyslexia and formal-dysgraphia
* Speech disorders (dysphasia, aphasia)
* Delayed development (pre-school)
* Minimal brain injury (MBI)
Figure
5.
(*Authors
of the original Hungarian book "Basic Therapy", Scientific Study,
Basic Therapy Foundation, Budapest 1999.:
1) Éva Marton-Dévényi M.D., Leader of the Basic Therapy Foundation;
2) Márton Szerdahelyi M.Ed., PT., Basic Therapy Foundation;
3) Gábor Tóth M.Ed., Basic Therapy Foundation
4) Katalin Keresztesi Ph.D., Assistant Professor, Hungarian University of
Physical Education, Faculty of Athletic.)
[index]